




.webp)
Ask any nurse, care coordinator, or hospital administrator why they got into healthcare, and you will not hear "to make reminder calls." You will not hear "to chase down prescription refills" or "to manually track which patients had their post-discharge follow-ups scheduled." They got into this to care for people, to be present at the moments that matter, to apply clinical judgment, to make someone's worst day a little more manageable.
But somewhere between that aspiration and the actual workday, something went wrong.
Today, a significant chunk of the healthcare workforce is buried in coordination work that has nothing to do with clinical expertise. A care coordinator starts her morning with a stack of discharge follow-up calls. A nurse spends part of her afternoon chasing pharmacy confirmations. A patient engagement team sends out the same refill reminders they sent last week and the week before.
By the time an actual patient interaction happens, the energy is already spent. The frustration is already there. And the patient on the other end, who just needs someone to talk to them like a human, gets the tired, transactional version of the professional who should be at their best.
This is not a staffing problem. Hiring more people does not fix it. It is a structural problem, and it compounds quietly every single day into something that shows up very visibly on the balance sheet.
Read more - Agentic AI in healthcare
The cost of poor care coordination: Medication non-adherence, care gaps, and missed follow-ups
Roughly 27% of 30-day hospital readmissions are avoidable. Not clinical failures. Not unavoidable tragedies. Avoidable, each one averaging $15,000 in cost that the system absorbs. Most trace back to a predictable cascade: a medication not picked up, a follow-up that fell through a scheduling gap, a warning sign that went unmonitored for four days because no one had the bandwidth to check.
Medication non-adherence alone costs an estimated $300 billion annually across the U.S. healthcare system. That number is not the result of patients refusing care. It is largely the result of patients losing their way through a process that asks too much of them at the worst possible moments.
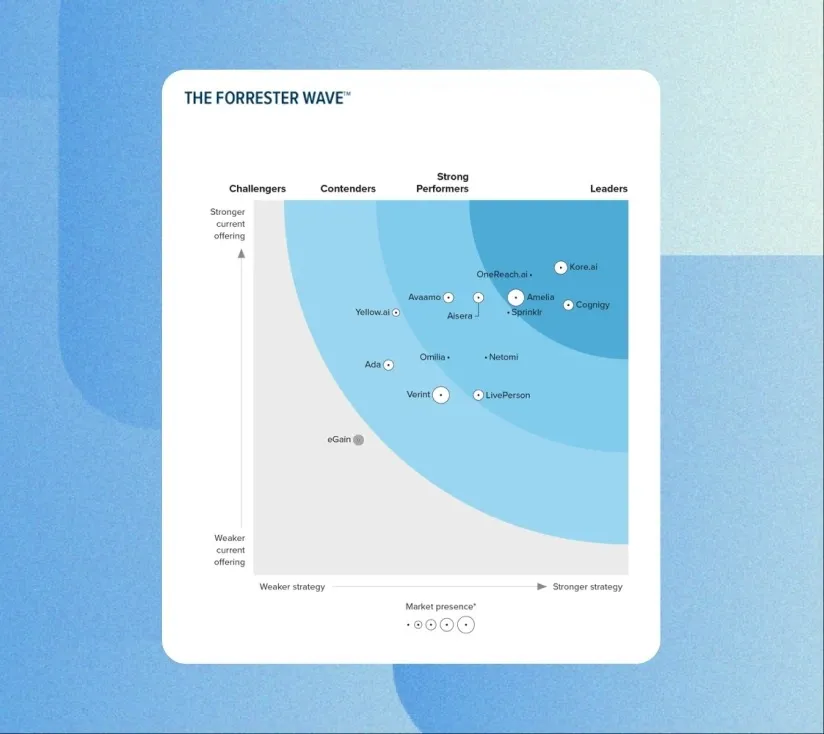
Meanwhile, over 80% of healthcare organizations are already prioritizing agentic AI for clinical operations and revenue cycle management, with 85% planning to increase investment over the next two to three years, according to research from the Deloitte Center for Health Solutions. Separately, research from Microsoft and the Health Management Academy, published in the New England Journal of Medicine, finds that while strategic interest is rising rapidly, most health systems remain in early stages, with 43% piloting or testing agentic AI but only 3% having deployed agents in live workflows. Deloitte's 2026 US Health Care Outlook reinforces the broader momentum: the majority of healthcare executives expect agentic AI to deliver moderate-to-significant value across clinical, operational, and patient-facing functions in the near term.
The question is no longer whether agentic AI belongs in healthcare operations. It is whether your organization captures the returns early, or spends the next few years watching the gap widen.
AI patient management automation: 24/7 follow-up available
What if the care coordinator could hand off every routine follow-up to something that never got tired, never forgot, and never let a patient fall through a gap, while she focused on the cases that actually needed her judgment?
That is the practical reality of agentic AI today.
Unlike traditional AI tools that surface an insight and stop there, agentic AI acts. It monitors. It follows up. It coordinates across systems without waiting for a human to initiate each step. A discharged patient does not just get a better discharge summary, they get a system that verifies the summary was acted on: that the prescription reached the pharmacy, the follow-up was scheduled, the first week of recovery stayed on track. And it does this across every patient, not just the ones who happen to call in on their own.
Think of it less like a smarter alert system and more like an endlessly scalable coordination layer that never drops the thread, without adding headcount.
AI-powered care coordination: Automated patient follow-up at scale
Post-discharge is where health systems lose the most ground, and where the intervention cost is lowest relative to the outcome.
Agentic AI turns that window into a structured, continuous workflow. Every patient receives follow-up calibrated to their specific diagnosis and recovery plan. Prescription fulfillment gets confirmed. Early warning indicators are tracked continuously. When something looks concerning, a care manager is alerted before it becomes an emergency admission.
The shift is from hoping follow-through happens to building a system where it is guaranteed.
Beyond readmissions, population health data already tells most health systems exactly which patients are overdue for preventive care. The intelligence is there. What has been missing is a scalable way to act on it without building a dedicated outreach function for every patient cohort.
Agentic AI handles the full loop, identifying the gap, triggering personalized outreach, coordinating scheduling, and escalating non-responders to a human team. Early real-world deployments are already showing measurable results. At Atlantic Health System, an AI agent deployed for colonoscopy outreach saw 39% of contacted patients confirm upcoming appointments within the first 30 days, while reducing staff time spent on those calls by 38%. At Geisinger Health System, AI-driven identification of high-risk patients due for colonoscopy increased screening completion rates by 30%, supporting earlier detection of colorectal cancer at more treatable stages.
For complex, high-acuity patients, think oncology, chronic disease management, multi-specialty coordination, agentic AI takes the administrative burden off the patient and returns 3 hours per week per complex case to clinical staff. Hours that go back to actual clinical work.
Agentic AI for health plans: Closing care gaps and improving HEDIS star ratings"
Health plans hold some of the most complete longitudinal member data in healthcare. Years of encounter history. Claims data that surfaces missed refills early and reliably. Patterns that predict complications months before they become costly events.
For too long, that intelligence has lived in dashboards that care management teams do not have the bandwidth to consistently act on. The insight exists. The action does not always follow.
Agentic AI closes that gap, automatically triggering personalized member outreach, coordinating in-network scheduling, and tracking care gap closure in real time across the full population. For organizations operating under value-based contracts, that closure rate is not a quality initiative in isolation. It is a direct lever tied to HEDIS scores, Star Ratings, and the revenue and penalties attached to both.
Organizations deploying agentic AI for care gap management are seeing 45% improvement in closure rates within 12 months of deployment.
The same logic applies to medication adherence. The data to catch a problem is already in claims. The challenge has never been detection, it is the distance between knowing and acting fast enough to matter. Agentic AI closes that distance, working with pharmacy partners to remove barriers before a missed refill becomes an inpatient admission.
30% improvement in medication adherence rates. 85% of adherence barriers resolved without clinical escalation.
Agentic AI for life sciences: Faster specialty therapy access and improved medication adherence
The path from "your doctor prescribed this" to "you are actually taking this medication" in specialty therapy is too long, too fragmented, and too easy to abandon.
Benefits verification. Prior authorization. Copay enrollment. Specialty pharmacy connection. Patient education. Every step is a potential exit point, not because patients do not want the therapy, but because the process asks too much of them at exactly the wrong moment.
Agentic AI transforms that gauntlet into a guided workflow, addressing every access barrier before it reaches the patient and maintaining engagement through the full arc of treatment.
35% faster time-to-first-fill. 40% reduction in patient dropout during the access phase.
And there is a longer-term return that tends to be undervalued: patients who stay engaged generate richer real-world evidence. For organizations increasingly operating under outcomes-based agreements with payers, that evidence becomes a strategic asset in every commercial and regulatory conversation for years.
How agentic AI improves care outcomes across providers, payers, and life sciences
Providers, payers, and life sciences companies tend to think of themselves as operating in separate lanes. But patients move through one continuous journey, and when any part of it breaks down, the costs ripple across all three.
When a health system reduces readmissions, the payer sees lower acute utilization. When a life sciences organization improves adherence, the provider sees better clinical outcomes and the payer sees fewer complications. When a health plan closes care gaps proactively, the provider benefits from more engaged patients and the life sciences organization sees stronger real-world therapy performance.
- Providers reduce readmissions > Payers see lower hospitalization costs
- Payers close care gaps > Providers see better-managed, more engaged patients
- Life sciences improve adherence > Providers see better outcomes; Payers see fewer complications
- All three generate cleaner real-world evidence > stronger outcomes-based contract performance across the board
Agentic AI is what makes cross-organizational continuity operationally possible at scale, not by replacing clinical judgment, but by ensuring no patient falls through a gap while everyone is looking elsewhere.
Healthcare agentic AI implementation: HIPAA compliance, EHR integration, and health equity
The deployments that deliver results share a common foundation. The ones that disappoint tend to skip the same steps.
Clinical governance and auditability. Every action an agent takes in a patient's care pathway must be traceable and grounded in clinical protocol. Human escalation is not a fallback, it is a designed workflow element that needs to be built in from day one, not retrofitted after something goes wrong.
Patient transparency. Patients need to understand what is acting on their behalf and why. This is not just a compliance consideration, it is the foundation of the trust that determines whether the engagement program actually engages anyone.
Health equity by design. A deployment that only works smoothly for digitally fluent, English-speaking patients does not close care gaps. It redistributes them onto the populations already most underserved. Multilingual support, accessibility across literacy levels, and deliberate design for limited digital access are not optional.
HIPAA compliance as infrastructure, not retrofit. Agentic systems operating on protected health information require zero-trust data architecture and full audit trails built in from the ground up.
Real integration depth. An agentic AI that communicates with patients but cannot read or write back to the EHR is generating noise, not care. The real measure is whether patient-facing actions are grounded in, and reflected in, the systems of record that govern care delivery.
Kore.ai AI for Healthcare: Scalable care coordination and patient engagement automation
Kore.ai operates as an intelligent coordination layer across the EHRs, RCM systems, payer portals, and communication channels that healthcare organizations already rely on, without requiring infrastructure replacement.
Its multi-agent orchestration engine coordinates end-to-end workflows across scheduling, clinical documentation, payer platforms, and pharmacy channels without manual handoffs. Agents process structured EHR data, unstructured clinical notes, faxed documents, and live voice and chat interactions with equal fluency. Prebuilt healthcare accelerators for eligibility verification, appointment management, benefit clarification, and follow-up coordination compress deployment timelines from months to weeks. The platform operates within HIPAA, SOC 2 Type II, HITRUST, and ISO 27001 frameworks, with every agent action logged, traceable, and auditable.
$3.2M in revenue enabled, California health system. Rising call volumes, complex multilingual demands, and staffing constraints were making consistent patient access impossible to sustain. Kore.ai automated routine interactions across appointment scheduling, lab inquiries, pharmacy refills, and referral management, adding multilingual after-hours coverage without adding headcount. The outcome was $3.2M in revenue enabled through automated scheduling alone, alongside significant reductions in operating costs and handle times.
Consistent member experience at scale, U.S. health plan, 12M+ members. The member journey looked different depending on which channel someone used, which representative they reached, and what time of day they called. Kore.ai unified automated self-service and live agent interactions across web, mobile, voice, and chat into one orchestrated environment, delivering consistency at scale, with analytics-driven visibility to keep improving over time.
Lower handle times, better multilingual accuracy, North American payer. Rising call volumes and manual documentation burden were stretching representatives and degrading service quality. Kore.ai delivered a phased transformation, starting with automation for high-volume routine interactions, adding transcription and summarization, then layering in real-time intelligent agent assistance during live calls. Handle times fell. Multilingual accuracy improved. The organization built the operational foundation for a fully agentic member services model that compounds in value as it scales.
In each case, Kore.ai did not ask organizations to rebuild what they already had. It worked within the existing environment, connected what was already in place, and delivered returns that grow stronger over time.
Read more - Kore.ai AI in heathcare
The Window Is Open. It Will Not Stay That Way.
The organizations that lead in patient management over the next five years will not necessarily be those with the most advanced clinical technology. They will be the ones who figured out how to make the system surrounding clinical care work as reliably as the care itself.
For health systems, that means fewer readmissions, stronger preventive care performance, and clinical staff doing clinical work. For health plans, it means proactive member engagement, better quality scores, and lower total cost of care. For life sciences organizations, it means faster patient access, stronger long-term adherence, and real-world evidence that holds up in every payer and regulatory conversation.
The patients moving through these improved systems will not know what agentic AI is. They will just notice that someone followed up. That their prescription was actually ready. That, for once, the system seemed to be working for them.
That is the outcome worth building toward. And the infrastructure to build it exists today.
FAQs
Q. What is the difference between agentic AI and traditional healthcare AI?
A. Traditional healthcare AI analyzes data and surfaces insights at a point in time. Agentic AI takes coordinated action across systems and timeframes, sequencing multi-step workflows, monitoring outcomes continuously, and escalating to humans when judgment is required. It does not just identify a care gap. It closes it.
Q. How does agentic AI improve patient engagement and adherence?
A. By making engagement proactive, personalized, and continuous rather than reactive and generic. Agentic AI monitors patient behavior across systems, detects gaps before they become clinical events, reaches patients through their preferred channels, and coordinates the support needed to resolve barriers, without requiring patients to navigate the process themselves.
Q. Is Kore.ai HIPAA compliant?
A. Yes. Kore.ai operates within HIPAA, SOC 2 Type II, HITRUST, and ISO 27001 frameworks, with full audit trails for every patient-facing action taken by an agent.
Q. What ROI can healthcare organizations expect?
Results vary by use case and deployment maturity. Organizations consistently report 22% reductions in 30-day readmissions, 45% improvements in care gap closure rates, 30% improvements in medication adherence, and 35% faster time-to-first-fill for specialty therapies.
Q. How long does deployment typically take?
A. With Kore.ai's prebuilt healthcare accelerators, organizations can move from pilot to live patient-facing workflows in weeks rather than months, depending on integration complexity and governance readiness.